Nexus Letter for Anxiety for VA Disability Claims


Quick Summary
- Anxiety can be service-connected even without in-service documentation, as long as the stressor or triggering event occurred during military service.
- Unlike PTSD, anxiety can result from accumulated operational stress or environmental factors rather than discrete traumatic events.
- Aggravation (pre-existing anxiety worsened by service) and secondary service connection (anxiety caused by a service-connected physical condition) are two distinct pathways requiring different evidence.
- Veterans already service-connected for anxiety but underrated can pursue increases based on current functional impairment documentation.
- Most anxiety claim denials result from insufficient nexus documentation or underdocumented functional impairment — not from the condition being unreal.
- What the VA Is Looking For in an Anxiety Claim
- Three Anxiety Claim Pathways: Direct, Aggravation, and Secondary
- When Anxiety Is Direct Service Connection or Aggravation
- Why Anxiety Claims Are Commonly Denied
- Already Service-Connected for Anxiety But Rated Too Low?
- IME Necessity Score
- Nexus Letter vs. Psychological IME
- What a Psychological IME for Anxiety Includes
- When You May Not Need a Psychological IME
- Frequently Asked Questions
Dr. Willoughby & Associates is a practice of licensed PhD and PsyD psychologists who conduct psychological Independent Medical Examinations for veterans pursuing VA disability claims. We have a direct interest in this topic, and we want to name that clearly.
Our position is not that every veteran with anxiety needs a full IME. When service treatment records clearly document the condition and a strong nexus is already established, simpler evidence may be sufficient. This article is written to help inform that decision, not to make it for you.
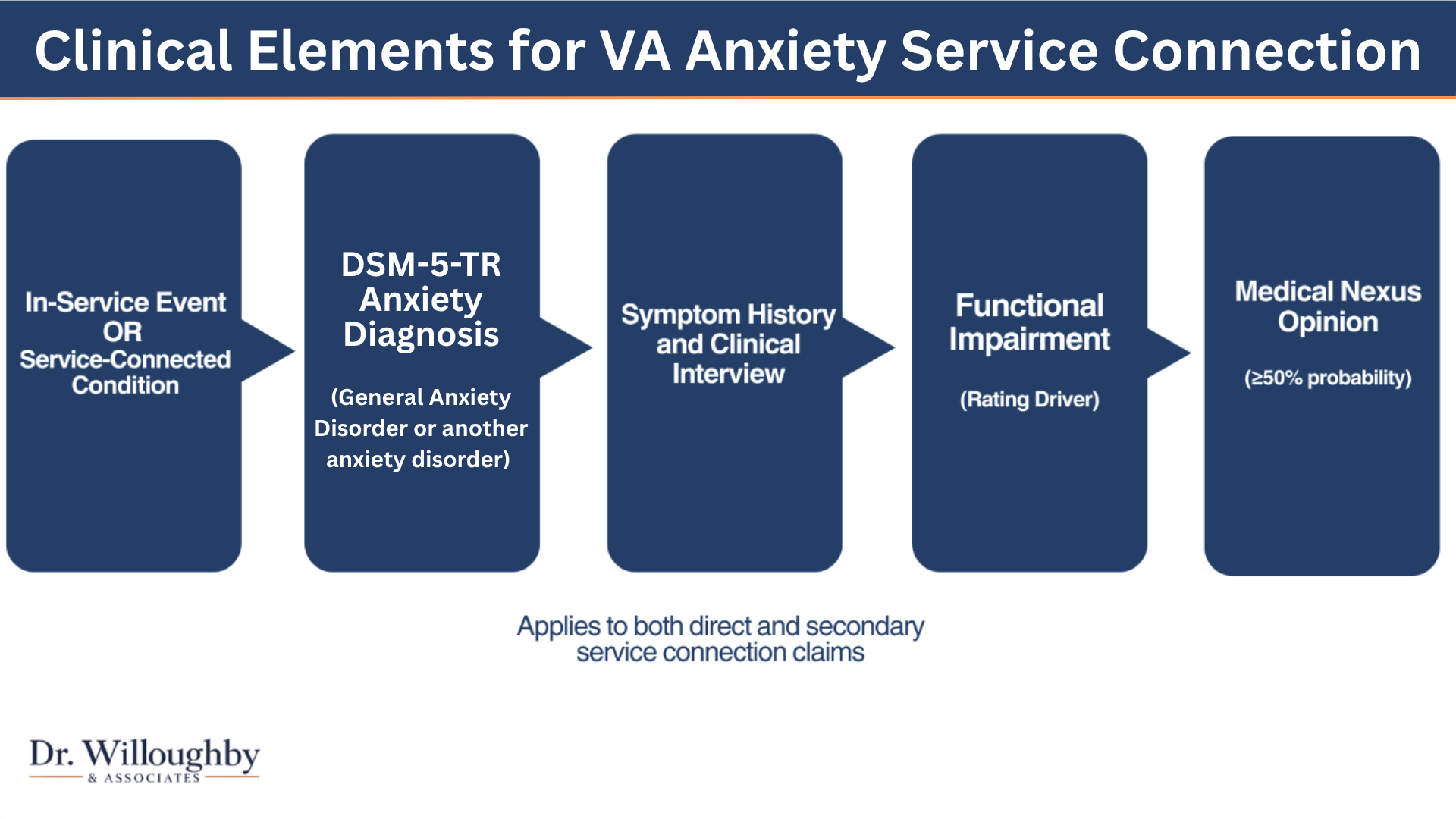
What the VA Is Looking For in an Anxiety Claim
Anxiety is one of the most commonly claimed, but inconsistently documented mental health conditions in VA disability claims.
The VA requires three things: a current diagnosis, proof of service connection, and documented functional impairment. Without all three, a claim gets denied even if the anxiety is real.
Current DSM-5 Diagnosis
Generalized Anxiety Disorder or another anxiety disorder, formally assessed. A diagnosis may be established during a comprehensive evaluation if one has not been received prior.
Service Connection Proof
Either something that happened during military service that caused anxiety, or documented evidence that pre-existing anxiety was aggravated by military service.
Medical Nexus with Reasoning
The link between anxiety and service must be explained, not just stated. The medical reasoning is what gives an opinion probative value under 38 CFR §3.159.
Functional Impairment Documentation
How anxiety affects the ability to work, maintain relationships, and manage daily life. This is the primary factor in your disability rating, not the diagnosis itself.
If you have an anxiety diagnosis and a military history, that is not enough on its own. Someone has to explain medically and in writing why those two things are connected and how your symptoms affect your daily functioning.
Three Anxiety Claim Pathways: Direct, Aggravation, and Secondary
Anxiety claims follow three distinct legal and clinical pathways. Each requires different evidence and documentation.
Direct Service Connection
Anxiety caused by military service.
The in-service stressor or event(s) must be documented or articulated, but a formal anxiety diagnosis during service is not required.
Examples: cumulative deployment stress, training-related anxiety, occupational demands during service that triggered anxiety.
Key: The stressor must have occurred during service.
Aggravation of Pre-Existing Anxiety
Pre-service anxiety worsened by military service.
Veteran had anxiety before service; military service made it significantly worse beyond its natural progression.
Examples: mild pre-service anxiety that became severe during deployment; anxiety at discharge that worsened substantially over time.
Key: Baseline + evidence of service-related worsening.
Pathway 3
Secondary Service Connection
Anxiety caused by a service-connected physical condition.
Anxiety develops from an already service-connected condition such as tinnitus, chronic pain, orthopedic injury, TBI, or migraines.
Example: A veteran service-connected for tinnitus develops anxiety because of chronic sleep disruption and functional impairment caused by the tinnitus.
Key: Medical evidence must explain the step-wise clinical progression under 38 CFR §3.310.
These three pathways are legally and medically distinct. Each requires different evidence and documentation. Direct connection focuses on the service stressor. Aggravation focuses on baseline anxiety and worsening. Secondary focuses on the step-wise progression from a primary condition.
Not sure which level of evidence your claim needs?
A free preliminary record review is the right starting point. A licensed psychologist reviews your file and tells you plainly whether stronger independent evidence is likely to help.
Request a Free Record ReviewNo fee. No obligation. No pressure to proceed.
When Anxiety Is Direct Service Connection or Aggravation
The Critical Distinction
Anxiety does not need to have been formally diagnosed or documented during service. What is required is that the stressor happened during service and can be articulated to a clinician during an interview.
During a clinical interview, you can describe:
- The operational environment and occupational demands
- Specific events or exposures that triggered anxiety
- Accumulation of stress over time
- Changes in performance or behavior during service that reflected anxiety-like symptoms
- Behavioral evidence: requesting transfer, substance use, performance deterioration, social withdrawal
Anxiety vs. PTSD: Why the Difference Matters
PTSD
Requires exposure to a discrete traumatic event meeting specific DSM-5 Criterion A criteria.
Anxiety
Can result from accumulated operational stress, environmental conditions, or gradual military stressors without requiring a single "trauma."
Clinical example: A veteran in a prolonged high-alert deployment may develop generalized anxiety from chronic hypervigilance demands, not from a specific traumatic incident. That is clinically valid and documentable.
Delayed Onset Is Valid — But Must Be Explained
Anxiety can appear months or years after separation if rooted in service-related stressors. Medical evidence must connect current symptoms to service events.
The clinician explains the timeline:
- Were there early mild symptoms during service that worsened over time?
- Did symptoms appear after discharge in response to life stressors that activated service-related patterns?
- How do the veteran's current symptoms relate to the in-service stressor?
Behavior Changes Count as Credible Evidence
Under 38 CFR §3.304, behavior changes following in-service stressors constitute credible evidence:
Occupational Changes
Requests for duty transfer, performance deterioration, discipline issues, or frequent job changes post-service.
Substance Use
Initiation or escalation of substance use during or after service as a coping mechanism.
Social Withdrawal
Documented relationship changes, social isolation, or unexplained relationship deterioration.
Symptom Markers
Anxiety symptoms without an identifiable cause (per regulatory language), or unexplained occupational/social behavior changes.
A clinician exploring your service history can identify these patterns and explain them as manifestations of anxiety.
Baseline and Worsening: What Aggravation Requires
Baseline Anxiety Before Service
Documented or articulated anxiety history prior to service. Examples: anxiety in high school, treatment prior to service, family history, discharge exam noting "occasional anxiety."
Documented Worsening During Service
Medical records or your articulation showing anxiety became significantly worse. This is not mild fluctuation. It is worsening that goes beyond what would naturally occur.
How Professional Judgment Works in Aggravation Claims
A clinician does not require a "before and after" side-by-side medical record. Professional judgment uses:
- Your description of pre-service anxiety levels and severity
- Treatment history (if any)
- What was presented during discharge examination
- How anxiety progressed post-service
- What circumstances in service would logically have worsened anxiety
The clinician then reasons: Given what we know about anxiety as a condition and what we know about this veteran's history, is it more likely than not that service aggravated this anxiety beyond its natural progression?
For Pre-Existing Anxiety, the Key Issue Is Service-Related Worsening
Under 38 CFR §3.310(a), the VA compensates aggravation claims when pre-existing conditions are worsened by military service. The compensation covers only the worsening attributable to service, not the pre-existing baseline.
Direct service connection requires that service caused the anxiety. Aggravation requires that anxiety existed before service and service made it worse. Both are valid pathways. Professional judgment helps bridge gaps in documentation.
Free Interactive VA Mental Health Evidence Review
Answer 6 brief questions to understand whether your file may need stronger independent medical evidence. No email required to view your result.
Why Anxiety Claims Are Commonly Denied
Most denials come down to evidence gaps. All of them are addressable.
Insufficient Nexus Opinion
Anxiety symptoms are documented, but no medical opinion connects them to service. The VA cannot grant service connection without competent medical evidence under 38 CFR §3.159.
Template or Conclusory Letter
The VA has increased scrutiny of formulaic opinions that state a conclusion without explaining reasoning. An opinion without documented rationale carries less probative weight.
No DSM-5 Diagnostic Formulation
Treatment notes and symptom reports are not the same as a formal diagnostic assessment. VA raters look for evidence that anxiety criteria were specifically evaluated.
Underdocumented Functional Impairment
Ratings are determined by how symptoms affect occupational and social functioning. Claims that establish service connection but do not document functional impact often receive lower ratings.
Minimization in C&P Exams
Veterans often minimize anxiety during C&P exams due to avoidance behaviors or somatic focus. A brief exam may miss the full picture of occupational and social impairment.
How Anxiety Presents Quietly in Exams
Anxiety often goes unrecognized during brief evaluations:
- Somatic symptoms (racing heart, tremor, GI distress) documented as "physical" complaints without anxiety label
- Avoidance behaviors read as "quiet" or "withdrawn" rather than symptomatic
- Occupational avoidance (avoiding certain duties, job-hopping) not connected to anxiety
- Relationship withdrawal attributed to personality rather than symptoms
A full clinical interview gives space to explore these patterns. A brief C&P exam often misses them.
Most anxiety claim denials are not because the condition is unreal. They are because the connection to service is not clearly explained, or the functional impact is not documented. Those are fixable problems.
Already Service-Connected for Anxiety But Rated Too Low?
If you are already service-connected for anxiety but your rating is 0%, 10%, or 30%, you may have a pathway to increase your rating based on current functional impairment documentation.
Key difference: This is about "how impaired are you now?" not "is anxiety service-connected?" The evidence focuses on current functional impact.
VA Ratings Are Based on Functional Impairment, Not Diagnosis Alone
Mental health ratings under 38 CFR §4.130 are determined by occupational and social impairment, not by the diagnosis itself.
Examples of impairment that support higher ratings:
- Job loss or frequent job changes due to anxiety
- Inability to maintain consistent employment
- Significant relationship deterioration
- Difficulty concentrating or completing tasks reliably
- Panic episodes triggering occupational or social avoidance
- Treatment changes (medication adjustments, therapy intensification)
Why Initial Ratings Are Often Incomplete
A C&P exam at initial claim may not have captured:
Post-Rating Changes
Anxiety that appeared or worsened after the initial rating
Employment Impact
Occupational impact (employment loss, job instability) post-rating
Social Deterioration
Relationship breakdown, isolation, or functional decline later
Treatment Intensity
Current treatment intensity or medication response changes
Evidence That Supports a Rating Increase
Updated Medical Documentation
Treatment records, therapy notes, or a psychological IME documenting current symptom severity and functional impact now.
Employment History
Documentation of job loss, frequent job changes, or inability to maintain work due to anxiety since the rating date.
Functional Impairment Analysis
Specific documentation of how anxiety currently affects occupational and social functioning using VA rating criteria language.
Private Psychological IME
A comprehensive evaluation focusing on current functional impairment with detailed nexus explaining the impact of anxiety now.
Two Ways to Increase Your Rating
Supplemental Claim
File new evidence showing worsening since the initial rating (employment loss, treatment intensification, functional deterioration). New medical evidence is permitted and encouraged.
Higher-Level Review
Request a senior VA reviewer re-evaluate your case using the same evidence in your current file. No new evidence needed; the reviewer uses existing documentation to determine if a higher rating is warranted.
Nexus Letter vs. Psychological IME — What the Difference Means for Your Claim
Not all medical opinions carry the same evidentiary weight. The VA evaluates probative value; how thoroughly documented and well-reasoned the opinion is.
| Criterion | Nexus Letter | Psychological IME |
|---|---|---|
| Length | ⚠ Typically 1–2 pages | ✓ 5–8 page comprehensive report |
| Clinical Interview | ⚠ Often not included | ✓ 50–90 minutes, structured |
| DSM-5 Diagnosis | ⚠ Often not formally documented | ✓ Yes, when clinically indicated |
| Medical Rationale | ⚠ Varies — often limited | ✓ Fully documented with clinical reasoning |
| Functional Impairment | ⚠ Rarely documented in depth | ✓ Detailed narrative analysis |
| Meets 38 CFR §3.159 | ⚠ May not fully document VA criteria | ✓ Yes, with documented rationale |
| Evidentiary Weight | ⚠ Typically lower than a full IME | ✓ Most comprehensive |
| Appeal Strength | ⚠ Often less robust | ✓ Most comprehensive |
Key point: Every IME includes a nexus opinion. Not every nexus letter reflects an IME-level evaluation.
A nexus letter states the opinion. A psychological IME shows the work behind it: the clinical interview, diagnostic assessment, records review, and the reasoning that connects the evidence to the conclusion. VA adjudicators and appeals boards weigh that documented work when opinions conflict.
For a full comparison that includes Disability Benefits Questionnaires and the complete evidence weight hierarchy, see our guide to VA mental health nexus letters and how they compare to other evidence types.
What a Psychological IME for Anxiety Includes
At Dr. Willoughby & Associates, all evaluations are conducted by W-2 licensed PhD and PsyD psychologists; employees of our practice, not contractors.
Records
Free Preliminary Record Review
A licensed psychologist reviews your service and medical records and tells you plainly whether stronger independent evidence is likely to help. No fee. No obligation.
Evaluation
50 to 90 Minute Clinical Interview
A structured evaluation conducted by a licensed psychologist via HIPAA-compliant telehealth. A full clinical interview exploring in-service experience, stressor history, symptom onset, and functional impact.
Diagnosis
DSM-5-TR Diagnostic Assessment
A formal diagnostic assessment documenting how anxiety criteria are met. Integrated with the full records review to establish a complete clinical picture.
Report
Written Medical Opinion, Delivered in 7 to 10 Business Days
A five to eight page report with a clearly documented nexus opinion and medical rationale structured to meet VA evidentiary standards under 38 CFR §3.159. Ready to submit with your claim or appeal.
Not sure which level of evidence your claim needs?
A free preliminary record review is the right starting point. A licensed psychologist reviews your file and tells you plainly whether stronger independent evidence is likely to help.
Request a Free Record ReviewNo fee. No obligation. No pressure to proceed.
When You May Not Need a Psychological IME
Not every anxiety claim requires an independent medical examination. An ethical provider will tell you that directly.
You May Not Need a Full Evaluation If
- Service treatment records already document anxiety symptoms and a continuous history
- Existing nexus evidence is well-reasoned and clinically documented
- A prior C&P exam was thorough and clearly supports service connection
- The claim involves a presumptive condition where a separate nexus opinion is not required
You May Need Stronger Independent Evidence If
- Your claim was previously denied
- A C&P exam was unfavorable or the rationale was thin
- Your condition is secondary to a service-connected condition
- Symptoms appeared years after separation with limited documentation
- You are preparing an appeal or supplemental claim
If the evidence already tells a clear story, you may not need anything additional. The preliminary record review is how to find out, before any time or money is spent on an evaluation that may not be necessary.
Secondary Service Connection: How Anxiety Develops from Physical Conditions
When anxiety develops from a service-connected physical condition, the medical evidence must show the step-wise clinical progression.
Example: How Physical Conditions Contribute to Anxiety
Primary Condition
Service-Connected Physical Condition
Tinnitus, chronic pain, orthopedic injury, migraines, or other recognized condition
Persistent symptoms interfere with sleep, daily functioning, and physical comfort over time
Mechanism Step 1
Chronic Functional Disruption
Sleep disruption, reduced activity, occupational stress, social withdrawal, loss of prior abilities
Sustained disruption contributes to emotional instability, worry, and psychological stress
Mechanism Step 2
Mood and Anxiety Dysregulation
Persistent anxiety symptoms, emotional instability, avoidance behaviors, worry escalation, reduced resilience
Meets DSM-5 diagnostic criteria when documented through clinical interview and records review
Secondary Condition
Generalized Anxiety Disorder
Meets DSM-5 diagnostic criteria when documented through clinical interview and records review
The pathway itself is not the medical opinion. It represents the clinical reasoning that must be documented through a structured interview, records review, and diagnostic assessment. A clinician explores your experience and explains how the primary condition contributed to the anxiety diagnosis.
For a comprehensive overview of all evidence types in mental health claims, including how different conditions compare, see our hub article on mental health nexus letters and independent medical examinations.
Frequently Asked Questions
Can anxiety be service-connected without in-service diagnosis or documentation? +
Yes. The stressor or triggering event must have occurred during service, but anxiety does not need to have been formally diagnosed or documented during service. It can be articulated during a clinical interview and the clinician can reason through how service events contributed to the current diagnosis.
What's the difference between anxiety and PTSD? +
PTSD requires exposure to a discrete traumatic event meeting DSM-5-TR Criterion A. Anxiety can result from accumulated operational stress, environmental conditions, or gradual military stressors without requiring a single trauma. Both are valid service connection pathways, but the evidence requirements differ.
Can I claim both anxiety and PTSD? +
Both conditions may be present, but the VA rates them under a single General Rating Formula for Mental Disorders (38 CFR 4.130) to avoid "pyramiding" — rating the same symptoms twice. A clinician documents both diagnoses, but the rating reflects overall mental health impairment, not separate percentages.
What if my anxiety developed years after service? +
Delayed onset does not disqualify a claim. The evaluation documents how the in-service stressor relates to current symptoms — tracing the connection even when significant time has passed. The clinician explains whether there were early symptoms that worsened, or whether symptoms appeared later in response to stressors that activated service-related patterns.
What's the difference between direct service connection and aggravation? +
Direct service connection means service caused the anxiety. Aggravation means pre-existing anxiety was worsened by service beyond its natural progression. They require different evidence pathways. Direct connection focuses on the service stressor; aggravation focuses on baseline anxiety and how much worse it became due to service.
What if my anxiety is caused by a service-connected physical condition like tinnitus or chronic pain? +
That is secondary service connection under 38 CFR §3.310. The medical evidence must explain the step-wise clinical progression from the primary condition to the anxiety. For example: tinnitus causes sleep disruption, sleep disruption contributes to mood instability, and mood instability manifests as anxiety disorder. See our guide to secondary service connection for detailed explanation.
What does "at least as likely as not" mean? +
A defined legal threshold — 50% or greater probability — under 38 CFR §3.159. The clinician does not need to say anxiety was definitely caused by service. Only that the connection is at least as likely as not, based on available evidence. This is the evidentiary standard required for VA disability claims.
Does a psychological IME guarantee my anxiety claim will be approved? +
No — and be cautious of any provider that suggests otherwise. Outcomes depend on many factors beyond any single piece of evidence, including your service history, other evidence in the record, and VA adjudicator decisions. What a comprehensive IME provides is the strongest possible medical foundation for your claim. We produce evidence. The VA makes decisions.
Related Educational Resources
Foundation
VA Mental Health Nexus Letters
What They Are, What They Are Not, and How They Compare to DBQs and Independent Medical Examinations
Read more →Decision Guide
Do I Need a Nexus Letter for My Claim?
When stronger independent medical evidence is likely to strengthen your claim or appeal
Read more →Secondary Pathway
Secondary Service Connection for Mental Health
How mental health conditions develop from service-connected physical conditions
Read more →Evidence Standards
What Is Competent Medical Evidence?
38 CFR §3.159 Explained — What the VA requires from medical opinions
Read more →IME vs C&P
Psychological IME vs. C&P Exam
Why the medical nexus and rationale matter in VA mental health claims
Read more →Condition-Specific
Nexus Letter for PTSD in VA Disability Claims
How the VA evaluates PTSD nexus letters, stressor documentation, and MST claims
Read more →About the Authors
Written By
Dr. Crystal Willoughby
PsyD, Licensed Clinical Psychologist
Founder. Maryland-licensed with extensive experience in psychological assessment and independent medical examinations for veterans nationwide, including anxiety, PTSD, depression, and trauma-related conditions.
Reviewed By
Dr. Amanda Barrow
PhD, Licensed Clinical Psychologist
Director of Veteran Services. Specializes in trauma-related mental health conditions and VA disability evaluations across the nation.
PSYPACT-certified telehealth — available in most U.S. states
This content is for educational purposes and does not constitute medical or legal advice.
Not sure which level of evidence your claim needs?
A free preliminary record review is the right starting point. A licensed psychologist reviews your file and tells you plainly whether stronger independent evidence is likely to help.
Request a Free Record ReviewNo fee. No obligation. No pressure to proceed.