Nexus Letter for Depression in VA Disability Claims: What the Evidence Must Show


Most depression claims are decided on how well the connection is explained — not whether the condition exists.
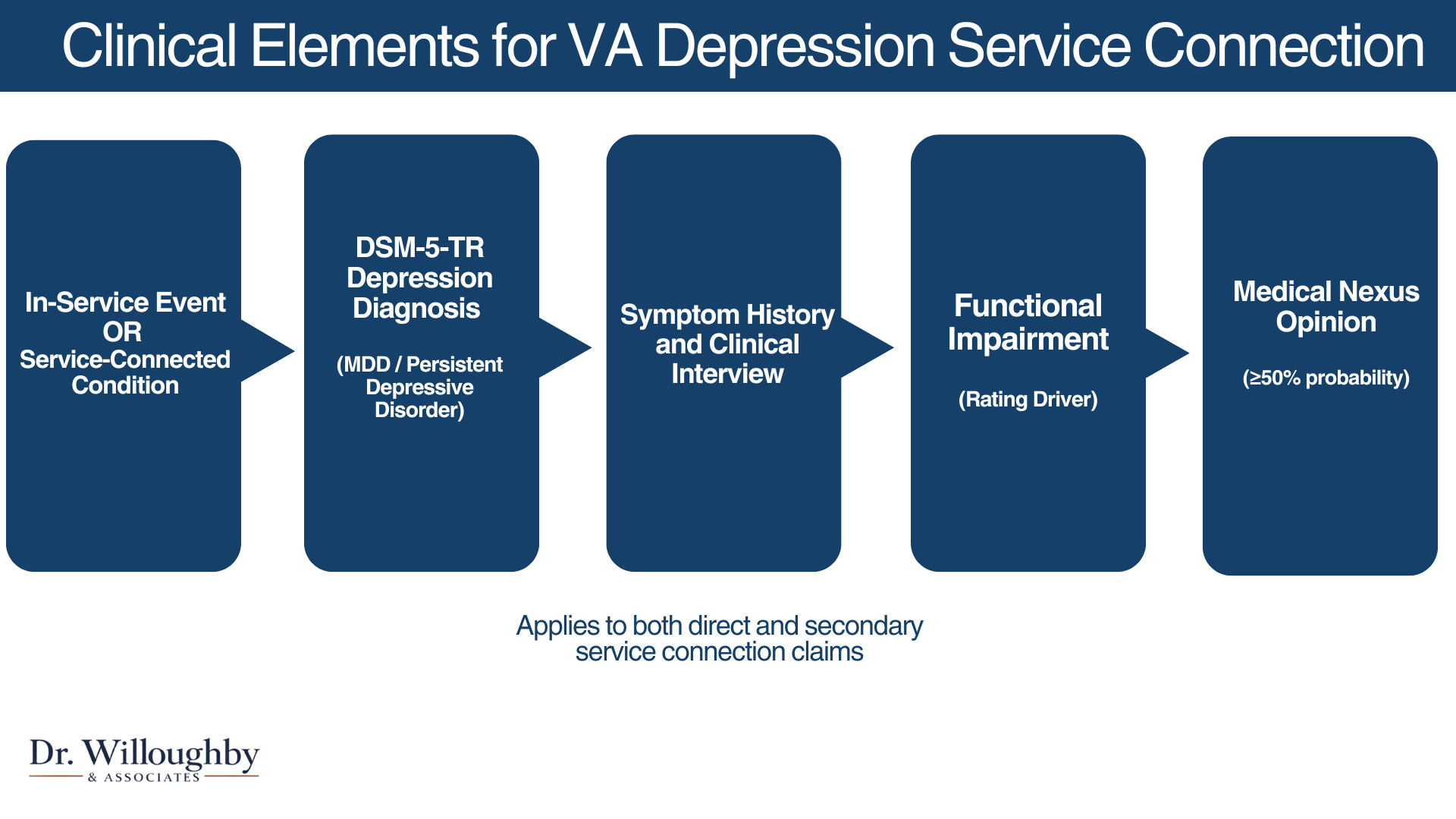
- Depression VA claims require three things: a current diagnosis, a connection to service or a service-connected condition, and a medical nexus explaining the link.
- The strength of that nexus — not just its existence — determines how much weight it carries with VA adjudicators.
- Functional impairment is a rating driver, not an afterthought. It needs to be documented specifically.
- Most depression claim denials aren't because the condition isn't real. They're because the medical reasoning wasn't clearly documented.
What the VA Is Looking For in a Depression Claim
Depression is one of the most commonly claimed — and commonly denied — mental health conditions in VA disability claims.
The VA is not simply looking for a diagnosis. It is looking for a documented medical nexus — a clinically supported link between your depression and your service — that meets the evidentiary standard under 38 CFR §3.159.
Understanding how that nexus evidence is evaluated is the foundation of any depression claim. Our guide to VA mental health nexus letters covers the full evidence framework.
Four things the VA evaluates in every depression claim
A current DSM-5-TR diagnosis
Major Depressive Disorder or persistent depressive disorder, formally assessed. A diagnosis may be established during a comprehensive evaluation if one hasn't been received yet.
A documented in-service event or service-connected condition
Either something that happened during military service, or an existing service-connected condition that contributed to the development of depression.
A medical nexus with clinical reasoning
The link between depression and service must be explained — not just stated. The reasoning behind the opinion is what gives it probative value under 38 CFR §3.159.
Functional impairment documentation — rating driver
How depression affects the ability to work, maintain relationships, and manage daily life. This is the primary driver of your disability rating — not the diagnosis itself.
If you have a depression diagnosis and a military history, that's not enough on its own. Someone has to explain — medically and in writing — why those two things are connected and how your symptoms affect your daily functioning.
Direct vs. Secondary — Two Paths, Different Evidence Requirements
Direct service connection
Depression developed as a result of something that happened during military service — combat exposure, MST, chronic operational stress, or a significant traumatic event.
Symptoms don't need to have appeared during service. What matters is that the originating event or condition occurred within that period.
Secondary service connection
Depression developed because of a condition that is already service-connected — such as chronic pain, tinnitus, PTSD, or TBI.
This includes cases where a pre-existing depression was worsened beyond its natural progression by a service-connected condition.
Already service-connected for tinnitus or a back injury? Depression that developed from that condition may qualify — but the connection has to be documented clinically, not just noted.
When Depression Is Secondary — What the Documentation Must Show
Secondary depression claims are where evidentiary gaps most commonly appear — and where a thorough clinical evaluation makes the most difference.
The VA requires the nexus opinion to explain the clinical connection, not just assert it. A letter stating "the veteran's depression is related to service-connected tinnitus" without supporting reasoning is vulnerable to being discounted.
A well-documented opinion traces the pathway:
Why Depression Claims Are Commonly Denied
Most denials come down to one of five evidence gaps — and all of them are addressable.
Missing or insufficient nexus opinion
The most common reason. Without competent medical evidence linking depression to service under 38 CFR §3.159, the VA cannot grant service connection regardless of how severe the condition is.
Template or conclusory letter
The VA has increased scrutiny of formulaic opinions that state a conclusion without explaining how it was reached. An opinion without documented rationale carries less probative weight.
No DSM-5-TR diagnostic formulation
Treatment notes and symptom reports are not the same as a formal diagnostic assessment. VA raters look for evidence that diagnostic criteria were specifically evaluated.
Unfavorable or limited C&P exam
A C&P exam that didn't fully capture symptom history or functional impairment can result in denial even when the underlying claim is valid. A private psychological IME provides additional competent medical evidence for the VA to consider.
Undocumented functional impairment
Ratings are determined by how symptoms affect functioning — not diagnosis alone. Claims that establish service connection but don't document impact often receive lower ratings than the veteran's actual impairment warrants.
Most depression claim denials aren't about whether the condition is real. They're about whether the medical evidence clearly explains the connection and documents the impact. Those are fixable problems.
Not sure what your file is missing? Dr. Willoughby & Associates offers a free preliminary record review.
Request a Free Preliminary Record Review — no fee, no obligation →Request a Free Preliminary Record Review No fee. No obligation. A licensed psychologist reviews your file.
Nexus Letter vs. Psychological IME — What the Difference Means for Your Claim
Not all medical opinions carry the same evidentiary weight. The VA evaluates probative value — how thoroughly documented and well-reasoned the opinion is.
When You May Not Need a Psychological IME
Not every depression claim requires an independent medical examination — and an ethical provider will tell you that directly.
An IME may not be necessary when:
- Service treatment records already clearly document the condition and a continuous symptom history
- Existing nexus evidence is well-reasoned and clinically documented
- A prior C&P exam was thorough and the rationale supports service connection
- The claim involves a presumptive condition where a separate nexus opinion isn't required
If the evidence already tells a clear story, you may not need anything additional. The preliminary record review is how we find out — before any time or money is spent on an evaluation that may not be necessary.
What a Psychological IME for Depression Includes
At Dr. Willoughby & Associates, all evaluations are conducted by W-2 licensed PhD and PsyD psychologists — employees of our practice, not contractors.
- 50–90 minute clinical interview
- Comprehensive review of relevant service and medical records
- DSM-5-TR diagnostic assessment
- Independent medical opinion with documented clinical rationale aligned with VA evidentiary standards
- Written report delivered within 7–10 business days, nationwide via HIPAA-compliant telehealth
Considering a Psychological IME for a Depression Claim?
At Dr. Willoughby & Associates, a licensed clinical psychologist reviews your file to determine whether a psychological IME may be clinically appropriate. There is no obligation to proceed. If the record does not support a medically defensible opinion, we will tell you that directly. The VA makes all claim determinations.
Request a Free Preliminary Record Review There is no fee for the review.Frequently Asked Questions
You need competent medical evidence under 38 CFR §3.159 connecting your depression to service or a service-connected condition. A nexus letter can satisfy that — but its strength depends on the clinical depth behind it. A brief conclusory letter carries less weight than a thoroughly documented evaluation.
Yes, but treating provider opinions are sometimes given less probative weight — both because the ongoing relationship may affect perceived objectivity, and because treating providers often aren't familiar with VA evidentiary language. An independent evaluation addresses both concerns.
A DBQ documents current symptom severity; a nexus opinion establishes the connection to service. A psychological IME typically addresses both in a single report.
Delayed onset doesn't disqualify a claim. The evaluation documents how earlier experiences or symptoms relate to current presentation — tracing the connection even when significant time has passed.
It's a defined legal threshold — 50% or greater probability — under 38 CFR §3.159. The clinician doesn't need to state that depression was definitely caused by service. Only that the connection is at least as likely as not, based on the available evidence.
No — and be cautious of any provider that suggests otherwise. Outcomes depend on many factors beyond any single piece of evidence. What a comprehensive IME provides is the strongest possible medical foundation for your claim.
PSYPACT-certified telehealth — available in most U.S. states
This content is for educational purposes and does not constitute medical or legal advice.