Secondary Service Connection for Mental Health Conditions in VA Disability Claims


- Secondary service connection applies when a mental health condition was caused or worsened by an existing service-connected condition — not directly by military service.
- Three elements are required: a current DSM-5-TR diagnosis, an existing service-connected condition, and a medical nexus explaining the relationship between them.
- The quality of the medical reasoning — not just the conclusion — determines how much weight the opinion carries with VA adjudicators.
Understanding Secondary Service Connection
Secondary service connection is a common pathway in VA disability claims.
It is also one of the most frequently misunderstood.
In VA disability law, secondary service connection refers to a condition that develops because of, or is worsened by, another condition that is already service-connected.
This pathway is especially relevant in claims involving mental health conditions.
Secondary service connection applies when a current condition was not caused directly by military service, but was caused or aggravated by a condition that already is service-connected.
Veterans sometimes refer to these as "VA secondary conditions" or "secondary disability claims."
For mental health conditions in particular, secondary service connection is one of the most frequently pursued — and most clinically complex — pathways in VA disability law.
If you've been service-connected for something like tinnitus or a back injury, and you've since developed depression or anxiety — there may be a pathway to connect that mental health condition to your existing rating. That's what secondary service connection means.
Legal Framework
What Secondary Service Connection Means in VA Disability Law
Secondary service connection is a legal and medical determination.
It requires establishing not only that a condition exists, but that a documented causal or aggravating relationship exists between that condition and an already service-connected disability.
Under 38 CFR § 3.310, a disability that is proximately due to or the result of a service-connected disease or injury shall be service connected.
The regulation also extends to aggravation — meaning a condition that existed prior to service, or developed independently, may still qualify if a service-connected condition has worsened it beyond its natural progression.
Direct vs Secondary Service Connection
Direct service connection establishes that a condition originated during military service.
Secondary service connection establishes that a condition originated from, or was made worse by, a condition that is already service-connected.
The distinction matters because the evidentiary requirements differ.
Direct claims typically focus on in-service records and continuity of symptoms. Secondary claims require an additional layer of medical reasoning — a documented explanation of how one condition contributed to the development or worsening of another.
The Role of Medical Evidence
In secondary mental health claims, medical evidence plays a central role.
The relationship between conditions is rarely self-evident from service records alone.
A veteran may have been service-connected for tinnitus for years before developing clinically significant anxiety or depression. The connection between those conditions requires clinical documentation that explains the mechanism — not just the co-occurrence.
Under 38 CFR § 3.159, competent medical evidence must come from a qualified professional and must include sufficient explanation for how the conclusion was reached.
The VA won't automatically connect your tinnitus to your anxiety just because both are in your file. Someone has to explain — medically and in writing — how one led to the other. That explanation is the nexus opinion.
What You Must Establish
The Three Elements Required for Secondary Service Connection
Secondary service connection for a mental health condition requires establishing three elements.
Each must be supported by the available evidence.
1. A Current Mental Health Diagnosis
The first element is a current, formally documented mental health diagnosis.
Under VA regulations, a diagnosis must meet the criteria set forth in the DSM-5-TR to be considered for rating purposes under 38 C.F.R. §§ 4.125 and 4.126.
A veteran's report of symptoms alone is not sufficient. The diagnosis must be established by a qualified clinician and documented in a manner consistent with VA evidentiary standards.
In some cases, veterans pursuing secondary mental health claims have not yet received a formal diagnosis. A comprehensive psychological evaluation can establish the diagnosis as part of the same evaluation that documents the nexus opinion.
2. An Existing Service-Connected Condition
The second element is an established service-connected condition — the primary condition from which the mental health condition is claimed to be secondary.
Common examples include:
- Tinnitus
- Chronic pain conditions such as back disorders, radiculopathy, or degenerative joint disease
- Traumatic brain injury (TBI)
- Other service-connected physical conditions that produce ongoing functional limitations
The primary condition does not need to be a mental health condition. In many secondary mental health claims, the primary condition is entirely physical.
3. A Medical Nexus Explaining the Relationship
The third element — and the one most often missing or insufficiently documented — is a medical nexus opinion that explains the relationship between the primary service-connected condition and the secondary mental health condition.
This opinion must do more than state that the two conditions are related.
It must explain the clinical mechanism connecting them. The VA evaluates the reasoning behind the opinion, not simply the conclusion.
A nexus opinion in a secondary mental health claim typically addresses:
- The nature and duration of the primary service-connected condition
- The clinical pathway through which the primary condition contributed to mental health symptoms
- The timeline of symptom development
- Whether the relationship meets the "at least as likely as not" threshold under 38 CFR § 3.159
Think of it as three boxes that all need to be checked: you have a diagnosis, you have an existing service-connected condition, and a qualified clinician has explained in writing how the two are connected. The third box is where most secondary claims run into trouble.
The VA evaluates the reasoning behind the opinion — not simply the conclusion.
Under 38 CFR § 3.159, competent medical evidence must come from a provider qualified through education, training, or experience.
The opinion must include sufficient explanation of how the conclusion was reached — not just the conclusion itself.
Opinions that address the clinical mechanism, symptom timeline, and record review are generally assigned greater probative value than those that state a conclusion without documented reasoning.
A denial doesn't close the door.
A psychological IME can support a supplemental claim or an appeal at the Board of Veterans' Appeals. This is one of the most common situations we evaluate — and one of the most important reasons to request a free record review before giving up on a claim.
Request a Free Record Review →Two Legal Theories
Causation vs Aggravation in Secondary Service Connection
Secondary service connection can be established through two distinct legal theories.
Understanding the difference is important because the medical evidence required to support each is somewhat different.
Direct Causation
Direct causation applies when a service-connected condition is the cause of the secondary condition — meaning the secondary condition would not have developed, or would not have developed in the same way, without the primary condition.
In a mental health secondary claim, direct causation might apply when a veteran develops clinically significant depression or anxiety that can be traced to the onset and progression of a primary service-connected condition.
The medical opinion must explain why the primary condition is the cause — not merely a contributing factor — using clinical reasoning supported by the record.
Aggravation of an Existing Condition
Aggravation applies when a secondary condition existed prior to, or developed independently of, the primary service-connected condition, but the primary condition has worsened it beyond its natural progression.
Under 38 CFR § 3.310(b), the VA will only compensate for the degree of aggravation — the worsening attributable to the service-connected condition — rather than the condition in its entirety.
Aggravation claims in mental health are clinically complex because mental health conditions naturally fluctuate over time. A well-documented evaluation addresses the baseline trajectory of the condition and explains how the service-connected condition altered that trajectory in a measurable way.
If your anxiety existed before your service-connected condition got worse, you may still have a claim — but it needs to show that your service-connected condition made things measurably worse than they would have been on their own.
Clinical Patterns
Common Clinical Pathways in Mental Health Secondary Claims
Secondary mental health claims often follow identifiable clinical patterns.
Understanding these pathways helps explain why the medical reasoning must go beyond a simple statement of connection.
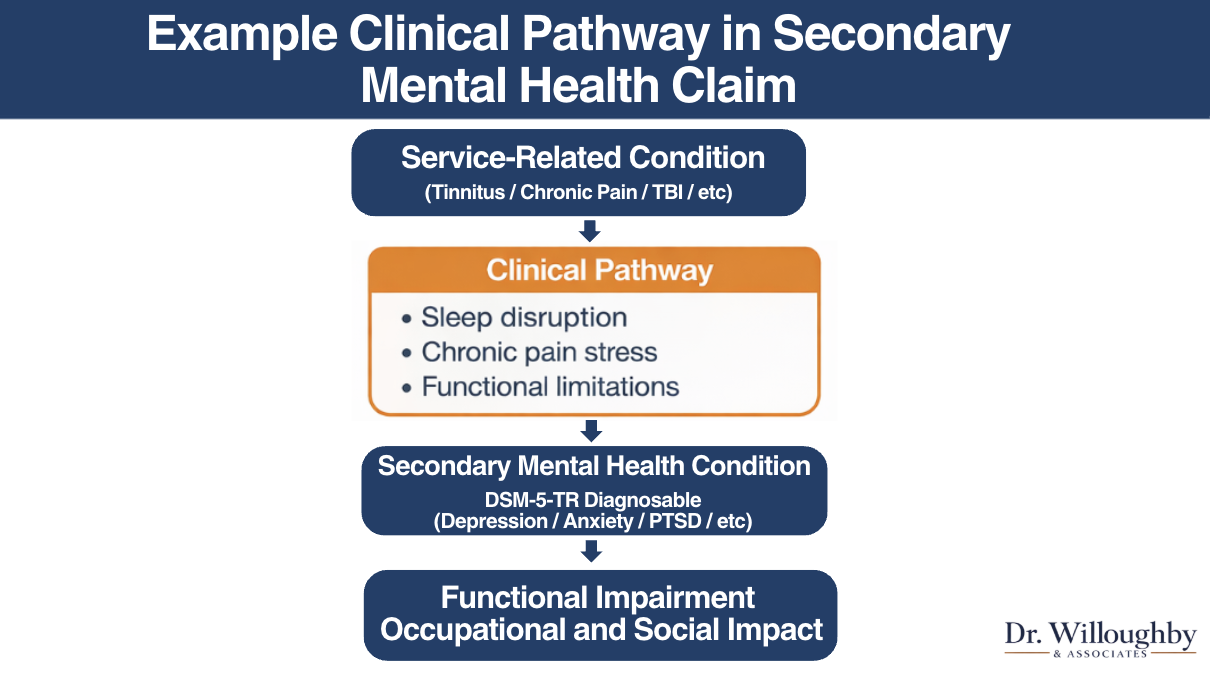
Primary Condition
Service-Connected Condition
Tinnitus, chronic pain, TBI, or other service-connected physical condition
Intermediate Step
Documented Clinical Progression
Sleep disruption, chronic stress, functional limitations, social withdrawal
Secondary Condition
DSM-5-TR Diagnosable Mental Health Condition
Depression, anxiety, PTSD, or other diagnosable condition meeting VA evidentiary standards
VA Rating Impact
Functional Impairment — Occupational and Social
The degree of impairment in work, relationships, and daily functioning determines the disability rating
Chronic Physical Symptoms and Psychological Impact
Chronic physical conditions — particularly those involving persistent pain, functional limitation, or significant changes in daily life — are well-documented contributors to depression, anxiety, and related mental health conditions.
A veteran living with chronic pain from a service-connected back condition may experience a progressive narrowing of activity, social withdrawal, disrupted sleep, and erosion of occupational functioning over time.
These are not simply emotional responses to discomfort. They represent a documented clinical pathway in which a physical condition contributes to changes in mood, cognition, and behavior that meet DSM-5-TR diagnostic criteria.
Sleep Disruption and Emotional Regulation
Sleep disruption is a clinically recognized intermediate step in several secondary mental health pathways.
Service-connected conditions including tinnitus, chronic pain, and certain physical injuries commonly interfere with sleep.
Chronic sleep disruption is associated with impaired emotional regulation, increased irritability, reduced cognitive functioning, and heightened vulnerability to mood disorders.
When the medical evidence documents this progression — primary condition contributes to sleep disruption, sleep disruption contributes to mood dysregulation, dysregulation progresses to a diagnosable condition — the nexus opinion carries greater evidentiary weight.
Functional Impairment Over Time
Secondary mental health conditions often develop gradually.
Veterans may not recognize the relationship between a physical condition and emerging psychological symptoms, particularly when those symptoms develop over years rather than weeks.
A comprehensive clinical evaluation addresses this timeline directly — documenting when symptoms first appeared, how they progressed, and how that progression aligns with the history of the primary service-connected condition.
Under the VA General Rating Formula for Mental Disorders, disability ratings are based largely on how symptoms affect occupational and social functioning.
You don't have to connect the dots yourself. That's what the clinical evaluation does — it traces the progression from your service-connected condition through to your current mental health symptoms, step by step, in language the VA recognizes.
One states the conclusion. The other explains the pathway that supports it.
Common Primary Conditions
Examples of Conditions That May Contribute to Secondary Mental Health Symptoms
Secondary mental health claims can arise from a wide range of primary service-connected conditions.
The following represent some of the most common clinical relationships evaluated in psychological IMEs.
Tinnitus and Mental Health Conditions
Tinnitus is among the most commonly service-connected conditions in the veteran population, typically rated at 10 percent under VA Diagnostic Code 6260.
The clinical pathway typically involves persistent auditory symptoms contributing to sleep disruption, which in turn contributes to mood dysregulation and, in some cases, a DSM-5-TR diagnosable condition such as depression or anxiety.
The medical evaluation must document this progression through clinical interview, record review, and diagnostic assessment — not simply assert that tinnitus caused anxiety.
For a detailed explanation of how this pathway is evaluated, see our article on When Tinnitus Contributes to Mental Health Conditions in VA Disability Claims.
Chronic Pain and Mood Disorders
Chronic pain conditions — including service-connected back disorders, joint conditions, radiculopathy, and neuropathy — are among the most common primary conditions in secondary mental health claims.
The relationship between chronic pain and depression is well-established in the clinical literature.
The evaluation must address the nature of the pain condition, its impact on daily functioning, the timeline of psychological symptom development, and the clinical reasoning explaining how the physical condition contributed to the emergence of a diagnosable mood disorder.
For more on how nexus opinions address complex multi-condition claims, see our overview of VA mental health nexus letters.
Sleep Disorders and Mental Health Symptoms
Sleep disorders, including service-connected insomnia or conditions that significantly disrupt sleep, represent another recognized secondary pathway.
Chronic sleep disturbance is associated with increased risk of depression, anxiety, and other mood-related conditions.
When the primary sleep disorder is service-connected, and when medical evidence documents the clinical progression to a diagnosable mental health condition, secondary service connection may be supported.
Evidentiary Standards
How Medical Evidence Is Evaluated in Secondary Mental Health Claims
The strength of a secondary mental health claim rests significantly on the quality of the medical evidence supporting it.
VA adjudicators evaluate not only whether a nexus opinion was submitted, but how thoroughly the reasoning behind that opinion is documented.
DSM-5-TR Diagnostic Documentation
Under 38 C.F.R. §§ 4.125 and 4.126, mental health diagnoses in VA disability claims must conform to the DSM-5-TR.
A diagnosis that does not meet these criteria, or that is not documented in a manner consistent with VA standards, may be given reduced weight by VA adjudicators.
The diagnostic documentation must establish not only the diagnosis but the clinical basis for it — the symptoms present, their duration and severity, and how they meet the diagnostic threshold.
Clinical Rationale and Symptom Timeline
The clinical rationale in a secondary mental health opinion must explain the pathway between conditions, not simply state a conclusion.
Adjudicators at the regional office, Higher-Level Review, and the Board of Veterans' Appeals evaluate how clearly the medical reasoning connects the evidence to the conclusion.
A well-documented opinion addresses:
- The history and progression of the primary service-connected condition
- The timeline of mental health symptom onset and development
- The clinical mechanism connecting the two conditions
- How the available medical and service records support the conclusion
- Why the evidence meets the "at least as likely as not" standard
For a full explanation of how the VA weighs medical opinions, see our guide to competent medical evidence under 38 CFR § 3.159.
What a Psychological IME Includes
A psychological IME is a structured clinical evaluation designed to produce comprehensive medical evidence for VA review in secondary mental health claims.
Unlike a VA C&P exam, which is administrative and time-limited, a psychological IME documents the full clinical picture with the depth that appeals-level review requires.
A psychological IME for a secondary mental health claim typically includes:
- Review of relevant records — military service records, service treatment records, post-service medical records, and any prior VA decisions
- 50–90 minute clinical interview — a structured evaluation of symptom history, onset, progression, and functional impact
- DSM-5-TR diagnostic assessment — formal diagnostic evaluation when clinically indicated, documented to VA evidentiary standards
- Independent medical opinion — a written nexus opinion addressing the relationship between conditions, the clinical pathway, and the evidentiary basis for the conclusion
- VA-compliant written report — 5–8 pages, delivered within 7–10 business days, structured for review at the regional office and on appeal
The distinction between a brief nexus letter and a full psychological IME is not the conclusion — it is the documentation of the reasoning process itself.
A nexus letter states that a condition is "at least as likely as not" related to service. A psychological IME explains the clinical mechanism, the symptom timeline, the record review, and the diagnostic basis that supports that conclusion.
VA adjudicators and appeals boards evaluate both. The opinion that explains its work generally carries greater probative value.
A nexus letter says "yes." A psychological IME says "yes, and here's exactly why, with the records and clinical reasoning to back it up." The VA weighs both — but not equally.
One states where the analysis ends. The other shows the work that supports it.
Our Commitment
Evidence, Not Promises
Secondary service connection for mental health conditions is among the more clinically complex pathways in VA disability law.
The relationship between a physical condition and a mental health outcome requires more than a statement of connection.
It requires documented clinical reasoning that explains the mechanism, the timeline, and the evidentiary basis for the opinion.
A well-documented psychological IME does not guarantee a specific outcome.
Claim decisions depend on the full evidentiary record, VA adjudicator determinations, and factors beyond any single piece of evidence.
What a thorough evaluation provides is the clearest possible medical foundation for the claim.
This article is provided for educational purposes and does not constitute medical treatment or legal advice.
Frequently Asked Questions
Can I file a secondary service connection claim if my primary condition is physical, not mental health?
Yes. Many secondary mental health claims stem from physical service-connected conditions like tinnitus, chronic pain, or TBI. The primary condition does not need to be a mental health condition.
The medical evidence must explain how that physical condition contributed to the development or worsening of a diagnosable mental health condition — the mechanism, the timeline, and the clinical reasoning behind the connection.
What if I don't have a formal mental health diagnosis yet?
A comprehensive psychological evaluation can establish the diagnosis as part of the same evaluation that documents the nexus opinion. You do not need a separate diagnosis before scheduling an IME.
The evaluation establishes the diagnosis and the nexus opinion together, in a single VA-compliant report. This is one of the more common situations we encounter in secondary mental health claims.
How is secondary service connection different from direct service connection?
Direct service connection links a condition to military service directly — the condition began during service and has continued since. Secondary service connection links a condition to another condition that is already service-connected.
The evidentiary requirements are different. Secondary claims require a medical nexus opinion that explains the clinical mechanism connecting the two conditions — not just in-service records and continuity of symptoms.
Will a nexus letter be enough for a secondary mental health claim?
It depends on the quality and depth of the opinion. Brief nexus letters without detailed clinical reasoning often carry less probative weight than a full psychological IME, particularly on appeal.
The VA evaluates the reasoning behind the opinion, not just the conclusion. A psychological IME documents the clinical mechanism, symptom timeline, record review, and diagnostic basis — not just the nexus statement itself.
My claim was already denied. Is it too late to pursue a psychological IME?
No — and this is one of the most common situations we evaluate. A denial does not close the door.
A psychological IME can support a supplemental claim or an appeal at the Board of Veterans' Appeals. In many cases, the original denial was based on an insufficient or unfavorable C&P exam. A comprehensive independent evaluation provides the additional competent medical evidence the VA is required to consider.
Does Dr. Willoughby & Associates guarantee a rating or claim approval?
No — and we'd encourage caution with any provider that does. Claim outcomes depend on many factors beyond any single piece of evidence, including the full evidentiary record and VA adjudicator decisions.
What we provide is a thorough, clinically rigorous, VA-compliant report that gives your claim the strongest possible medical foundation. We produce evidence. The VA makes decisions.
Considering a Psychological IME for a Secondary Mental Health Claim?
If you are evaluating whether additional medical evidence may be helpful in your case, request a free record review consultation. Licensed clinical psychologists experienced in secondary mental health conditions will assess whether a psychological IME may be clinically appropriate.
Request a Free Record Review There is no fee for the review.Related Educational Resources
VA Mental Health Nexus Letters: What They Are and How They Compare
Read more → Nexus LetterDo I Need a Nexus Letter for a VA Disability Claim?
Read more → Secondary PathwayWhen Tinnitus Contributes to Mental Health Conditions
Read more → Evidence StandardsWhat Is Competent Medical Evidence? (38 CFR §3.159 Explained)
Read more → IME vs C&PWhy Strong Evidence Requires More Than a 20-Minute Interview
Read more → VA EvidenceUnderstanding Medical Evidence for VA Disability Claims
Read more →Written by
Dr. Crystal Willoughby, PsyD
Licensed Clinical Psychologist, Founder. Maryland-licensed with extensive experience in psychological assessment and independent medical examinations for veterans nationwide.
Reviewed by
Dr. Amanda Barrow, PhD
Licensed Clinical Psychologist, Director of Veteran Services. Specializes in trauma-related mental health conditions and VA disability evaluations.
Dr. Willoughby & Associates is a specialized Independent Medical Examination practice focused on veterans' mental health VA disability claims. Our licensed PhD and PsyD clinicians conduct full psychological IMEs nationwide via PSYPACT-certified telehealth. Visit our Education Hub for more resources on nexus letters, IMEs, and VA mental health claims.
PSYPACT-certified telehealth — available in most U.S. states
This content is for educational purposes and does not constitute medical or legal advice.